Research Results
Contributing to early discovery, supporting diagnosis by endoscopists
Immediate detection of colorectal cancer with AIFY2019

- Ryuji Hamamoto(Division Chief, Division of Molecular Modification and Cancer Biology, National Cancer Center Research Institute)
- CREST
- Development and Integration of Artificial Intelligence Technologies for Innovation Acceleration “Project on Development of Integrated Medical System for Diagnosis and Treatment of Cancer by Artificial Intelligence” Research Director (2016-2018)
- AIP Accelerated PRISM research
- “Development of the innovative drug discovery system using artificial intelligence“ Research Director (2018-2020)
Improved polyp detection to the detection rate of 98%
In joint research conducted with Doctor Masayoshi Yamada of the Department of Endoscopy, National Cancer Center Hospital, and NEC Japan, a CREST research director, Ryuji Hamamoto division chief, successfully developed a system (Figure 1) in 2017 that immediately detects colorectal cancer and ulcerative colon polyps, a precursor to cancer, during an endoscopic examination using artificial intelligence (AI). It automatically detects colorectal cancer and polyps from images and videos taken during an endoscopic examination of the colon, and aids in discovery of lesions by endoscopists. It improves polyp detection, which was an issue during such exams, and increases the detection rate. In this manner, it greatly contributes to the prevention and early detection of colorectal cancer.
Since the prototype of the developed diagnostic support system quickly provides feedback to physicians in the clinical setting, it operates on one computer using an advanced graphics processing unit (GPU) suited to image processing and its unique high-speed processing algorithm*1, based on AI technology, that utilizes deep learning well-suited to image processing. They used endoscopic images from approximately 5,000 cases of colorectal cancer and lesions from the Department of Endoscopy, National Cancer Center Hospital, and let the cutting-edge AI technology of NEC learn the data. They analyzed new endoscopic images by the AI after the learning, and obtained a 98% cancer detection rate (Figure 2). Furthermore, since the time it takes for detection and display of the results is extremely short (within 33 milliseconds*2 (30 frames per second)), they succeeded in realizing real-time display.
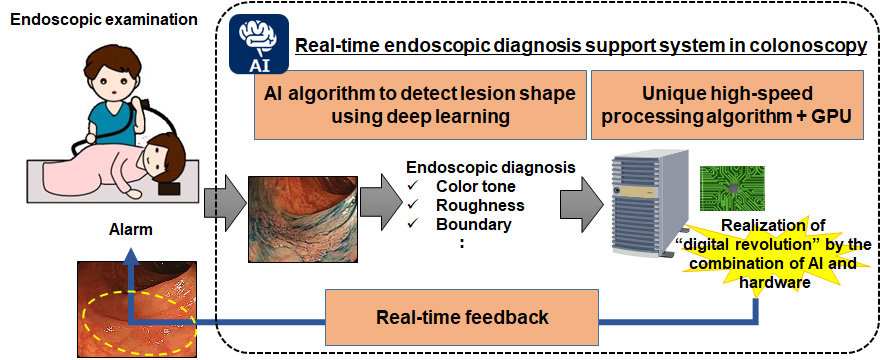
Figure 1. Real-time endoscopic diagnosis support system.
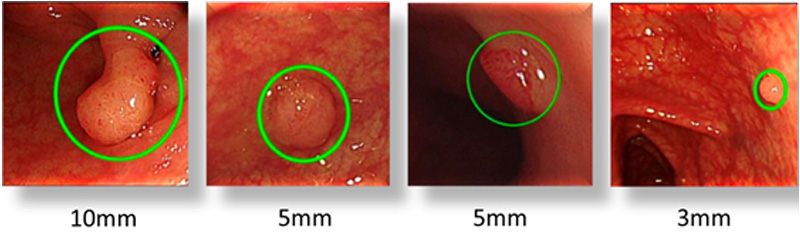
Figure 2. An example of polyp detection.
*2 1/1,000th of a second.
Lesion resection regulates prevalence and mortality
It is clear that polyps are a precursor to colorectal cancer. When polyps are found during medical checkups or colorectal cancer examinations, the polyps are endoscopically resected. According to the National Polyp Study (NPS) of the USA in 1993, and long-term data published by NPS in 2012, when polyps that require treatment (colorectal adenomatous polyps) are endoscopically resected, the prevalence of colorectal cancer can be reduced by 76–90%, and morbidity can be reduced by 53%.
Polyps are visually detected by endoscopists, but due to small sizes or unusual shapes, they might be overlooked. It has been reported that 24% of polyps are overlooked due to difficulty in terms of visual detection, occurrence sites, and differences in the skills of physicians (Figure 3). Another report states that 6% of cases develop colorectal cancer despite having undergone a colonoscopy. The causes for this were oversight during endoscopic examination (58%), not visiting the hospital (20%), new onset (13%), and insufficient endoscopic resection (9%).
Figure 3. The rate of oversite during colonoscopy.
Support for the limitations in the visual field, and instantaneous analysis of a large image space
By utilizing the newly developed real-time endoscopic diagnosis support system in colonoscopy, lesions that were previously difficult to detect can be detected more easily. It is especially effective in the upper end of the large intestine where flat lesions are difficult to detect. The detection rate for polyps is known as a parameter that indicates the quality of a colonoscopy; thus, the quality of endoscopists may also be improved.
In addition, since the real-time endoscopic diagnosis support system can analyze the whole image displayed by the endoscope, it is able to instantly analyze a much wider image space than conventional techniques. As a result, it supplements the limits of the human visual field, and further reduces oversight of polyps.
Even physicians with limited experience with colonoscopies could carefully observe the sites indicated by the real-time endoscopic diagnosis support system in addition to visible polyps, preventing oversight of cancers and lesions.
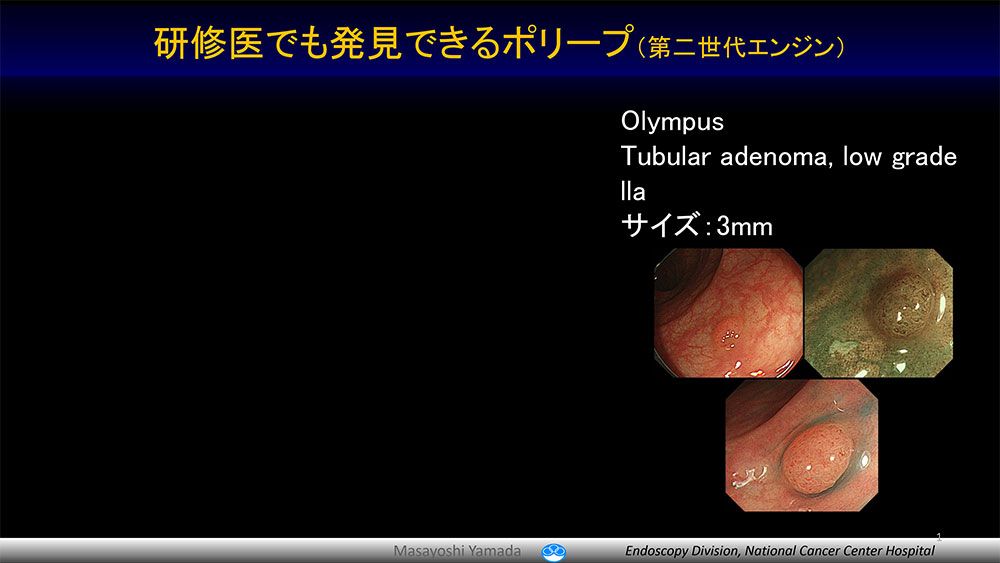
The polyp which even a resident training in endoscopy can detect (the second generation engine).
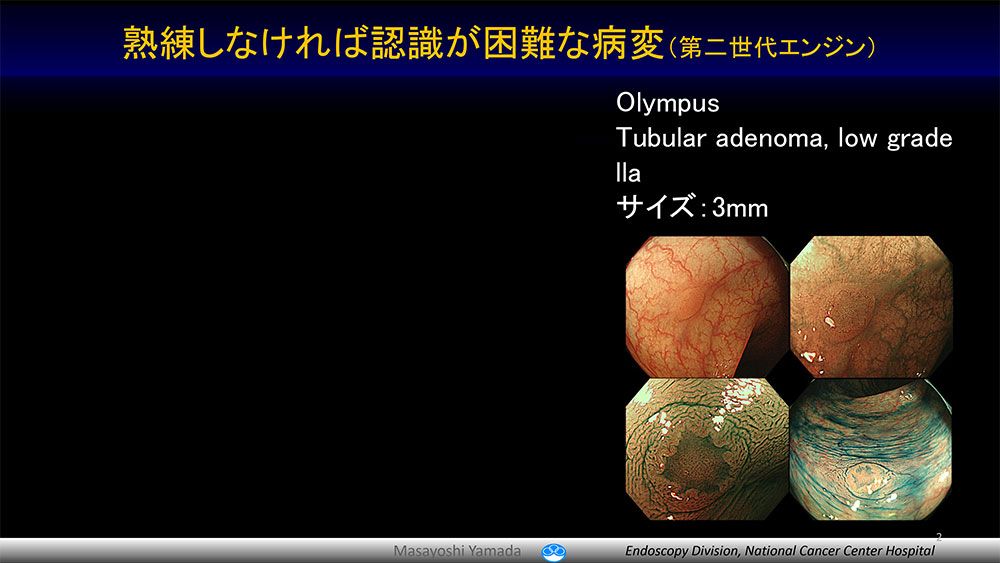
The lesion which an expert endoscopist can detect (the second generation engine).
Global commercialization through hospital-research laboratory collaboration
In the future, they plan to improve the accuracy of the prototype by having the AI learn over 1,600 flat and depressed lesions at National Cancer Center Japan that are difficult to detect with the naked eye. They are consulting PMDA and preparing clinical trials. By utilizing new endoscopes such as image enhanced endoscopes, they hope to learn detailed structures and patterns on the surface of colon polyps aimed at the qualitative diagnosis of intestinal polyps and prediction of lymph node metastasis of colorectal cancer. Furthermore, they are aiming to link with information such as CT images and molecular biology, and build a multi-modality real-time endoscopic diagnosis support system with even higher utility value.
The National Cancer Center Hospital and research laboratories are working together toward early clinical application as part of social implementation (Figure 4). Specifically, research will be further accelerated by connecting the AI analysis area at the National Cancer Center Japan and image recording server at the Department of Endoscopy, National Cancer Center Hospital. As AI learns flat and depressed lesions that are difficult to detect with the naked eye, the system accuracy will be improved. After clinical trials, they aim toward global commercialization.
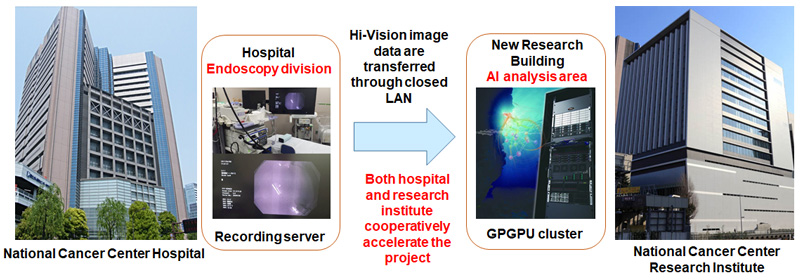
Figure 4. National Cancer Center Hospital and research laboratories are jointly accelerating the research toward early clinical application (social implementation).